
BIRTH MECHANISM IN OCCIPITAL PRESENTATION
The birth mechanism refers to the way the fetus and other parts of the gestational sac pass through the birth canal. The birth mechanism involves: birth forces, the birth passage, and the birth objects.
When the uterus contracts, the pressure in the uterine cavity is uniform everywhere. The weak point in the uterine wall is the cervix, so the contents of the uterus are pushed in this direction. Due to increased pressure in the uterine cavity, the amniotic membranes and amniotic fluid are pushed forward through the internal cervical os outward.
Cervical dilation is the result of two forces: downward pressure (hydraulic pressure) and upward traction. Pressure drives the amniotic sac into the cervix, while traction causes the muscles of the contractile portion to retract, the distensible portion of the uterus to stretch (distract), and the os to open. The contractile portion of the uterus becomes thicker, while the distensible portion becomes thinner. The uterus would pull completely over the fetus if it were not anchored in the pelvic cavity by ligaments and the vagina. Contractions also fulfill internal and external retraction. The uterine wall presses tightly against the abdominal wall muscles and pelvic muscles (external retraction); the fetal head adheres to the uterine wall at the contact ring (internal retraction).
The fetus must adapt to the birth canal due to its size and firmness. The deeper it descends into the pelvis, the more it is compressed circumferentially and the more cylindrical it becomes. It must curve to match the curvature of the birth passage. It must rotate so that the easiest curvature of a particular part of the fetal body corresponds to the pelvic curve (the line of direction). In the cervical region, the spine curves most easily forward or backward, while in the thoracic and lumbar regions it curves to the side.
Occipital presentation is the only correct cephalic presentation, because the fetus is born under the most favorable conditions (the first occipital presentation is more common and more favorable).

The longitudinally oval head engages in the transverse oval of the pelvic inlet and thus adapts to the available space.
Internal obstetric examination reveals that the sagittal suture runs in the transverse diameter of the pelvic inlet, usually not exactly midway between the symphysis and the sacral promontory, but closer to the promontory, because the promontory obstructs the entry of the posterior pelvis. If the sagittal suture is exactly midway between the promontory and the symphysis, we speak of synclitic engagement. If the anterior parietal bone enters first and the sagittal suture is closer to the promontory, we speak of anterior asynclitism or Naegele’s obliquity. This asynclitism is normal and disappears during labor, whereas posterior asynclitism or Litzmann’s obliquity is a serious abnormality (the posterior parietal bone attempts to enter first, and the sagittal suture is closer to the symphysis).
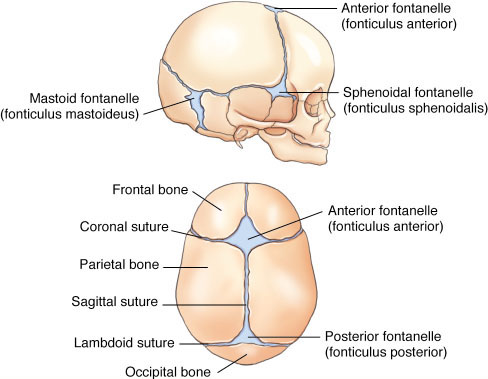
In asynclitic engagement, the cervical portion of the spine curves to the side. In the first occipital position, the posterior fontanelle is on the left and the anterior fontanelle on the right side. In the second occipital position, it is the opposite. As long as the head is not flexed, both are at the same height. When the head flexes, the posterior fontanelle descends lower and becomes the leading point of the head. It is slightly off the line of direction (eccentric). When the head flexes, it is born with the shortest (small oblique) diameter and the smallest (small) circumference, which is favorable for the course of labor.
We distinguish the birth mechanism of the head, shoulders, and the rest of the body.
BIRTH MECHANISM OF THE HEAD

- FLEXION – with contractions and abdominal pressure, pressure is transmitted from the fetal buttocks through the fetal spine to the head. The head flexes. The deeper the head descends, the more it flexes. The posterior fontanelle descends lower and becomes increasingly centered until it reaches the line of direction.
- DESCENT – the flexed head moves through the pelvic cavity until it reaches the mid-pelvis. The sagittal suture runs transversely, the posterior fontanelle is on the left in the first position, on the right in the second. It lies eccentrically and is the lowest point.
- INTERNAL ROTATION – when the head has reached the mid-pelvis, it begins to rotate internally while simultaneously moving to the pelvic floor. In the first position, it rotates so that the sagittal suture first runs in the right oblique diameter of the pelvic strait and finally in the longitudinal diameter of the pelvic outlet. The posterior fontanelle, which is initially on the left, moves first to the left front and finally under the symphysis. It is the lowest point. The anterior fontanelle is at the sacrum, higher than the posterior fontanelle. In the second position, the position is similar, only reversed. Internal rotation is the result of the longitudinally oval head adapting to the space. Internal rotation also occurs because the easiest curvature of the cervical spine adapts to the pelvic axis (line of direction). Another reason is the eccentricity of the posterior fontanelle, which, when moving forward, hits the lateral pelvic wall and rebounds forward.
- EXTENSION – on the pelvic floor, the head presses the occiput against the pubic arch and begins to extend over the perineum. First the occiput is born, then the vertex, forehead, and face. Extension is the result of pressure in the direction of the vertex. The pelvic floor muscles push the head toward the symphysis.
- EXTERNAL ROTATION – the already born head rotates externally, in the first position toward the mother’s right thigh, in the second toward the left thigh. External rotation is the result of internal rotation of the shoulders.
As the head moves through the pelvis, the shoulders must also move. When the head has reached the pelvic floor, the shoulders enter the pelvic inlet (the transverse diameter of the shoulders in the transverse or oblique diameter of the pelvic inlet). As the head is born, the shoulders move forward until they reach the pelvic floor. If the shoulders enter the pelvis in an oblique diameter, they pass through the opposite oblique diameter from the head. On the pelvic floor, the shoulders rotate internally so that the transverse diameter of the shoulders comes into the longitudinal diameter of the pelvic outlet. With internal rotation, the easiest curvature of the thoracic and lumbar spine adapts to the pelvic axis. The anterior shoulder (right in the first position, left in the second) then presses against the pubic arch, and the posterior shoulder is born over the perineum. When the shoulders rotate internally, the head rotates externally.
The fetal back remains on the left during birth in the first position, on the right in the second. Because it is born along the line of direction, it must curve strongly to the side. The spine curves more easily to the side in the thoracic and lumbar regions than forward or backward.
The buttocks enter with the transverse diameter in the longitudinal diameter of the pelvic inlet. They move through the pelvic cavity until they reach the pelvic floor. Internal rotation is absent. The anterior hip presses against the pubic arch, and the posterior hip is born over the perineum. It is possible for both hips to be born together. The birth of the legs follows.

Source: I believe the birth mechanism is still best explained in the book “Obstetrics” by Dr. Vito Lavrič (Ljubljana, 1959)


{kind=link}
{kind=link}
{kind=link}